
|
Three factors determine disease progression: Disease driver, WOB and mind. Disease driver is an independent process which initiates a disease and drives it. WOB
and mind are dependent processes,
particularly WOB which creates its solutions to minimize the damage
caused by the driver. In most chronic diseases,
disease driver is unknown. We shall start therefore with an infectious disease where the
driver is apparent.
The insets include a mathematical formulation of the ideas in this chapter.
|
Disease progression = R[i+1]
= R[D(i), W(i), M(i)] R : Resources |
Acute infection
Sore throat is driven by microbes. When
infection starts, WOB restructures
processes to meet the threat. On the local arena it mobilizes an inflammation, manifested by a locally elevated temperature, redness,
swelling and pain. These classical signs of infection were known to the ancient
Greeks and Romans like Celsus ( calor, rubor, tumor, dolor et functio laesa). They
actually have two meanings:
1. From WOB perspective they
are solutions to curb infection.
WOB first increases local blood flow (vasodilation), raising
the supply of resources to combat infection. This accounts for a local redness, swelling and warmth.
Pain stiffens muscles and makes
them still. Unnecessary muscular activity like swallowing might promote the
invader to other tissues. Fever, prostration, weakness, and the loss of appetite
are (systemic) WOB solutions. Some
microbes thrive less in elevated temperature. Weakness and prostration force
the patient to rest and save resources which are diverted to the throat.
2. These symptoms are also messages from WOB to the mind. Pain and discomfort, instruct the mind
to seek help. They are also messages
to the physician, indicating WOB state.
As long as WOB does not complain and there is no pain, physician may
watch and wait, since WOB still controls the new situation.
Treatment decision space
Physician has to decide when to interfere, and how vigorous treatment will
be. Treatment intensity and
timing are two parameters in his decision space. A decision space consists of a set of WOB signals and their appropriate treatments. The signal set consists of systemic and local signals like those
mentioned above. Each signal may be treated separately . Fever is reduced with aspirin, Gargles of cold water soothe the throat, and so on. Antibiotics
are the most effective. With all these options at hand, physician has to decide
when to start treating and how intense treatment will be?
|
Decision space
= DS(i+1) = {[m( i ), t( i, p)]} |
Infection is an experience
It seems reasonable to start treating an infection as early
as possible since the microbe population (D(i)) continually grows. However
such an approach ignores that
infection is an experience, which
teaches WOB how to cope with
it so that in the future it will handle it better.
Immunology distinguishes between innate and adaptive immune system. The first is inborn, while the second
learns from experience. However WOB experience us more than that. The
entire body learns from this
experience and not only the immune system.
WOB learns to respond more swiftly and efficiently. On the local arena, WOB learns to mobilize capillaries
(angiogenesis) more swiftly and
brings more resources to the scene. It may learn also how to withstand infection
at a lower temperature. Experience
teaches WOB how to create better solutions.
Infection trains WOB
Since infection trains WOB
to handle future infections better,
an effective training requires to
delay treatment. You might
compare this experience with athletic training, when your will (mind) becomes
the driver (D(i)) . The longer the daily training, the better the result. Athletic training is more than just muscle building. The
organism learns how to utilize
resources more efficiently and this is
also the essence of infection training.
You may notice that from WOB perspective the drivers (D(i)) of infection training
and athletic training are the same. WOB is unaware of the driver's nature. It regards drivers as a challenge for which it creates an optimal solution. "Driver" is a medical concept
to assist the physician in designing a therapy.
How long should
a therapy be delayed? It depends on the patient's condition. A
strong youngster may wait, while a fragile elderly ought to be treated sooner.
Influenza experience
Each year a flu epidemic sweeps
the globe and WOB has to handle an ever changing virus. Nevertheless
it gets smarter, since flu experience is more than
an immunological memory. Following every
flu WOB becomes more efficient.
Resistance and tolerance
In order to decide when to treat we need a measure of the patient's reserves,
which is called here tolerance, or resistance to a challenge. The French
philosopher Canguilhem defines health
as follows: . "Health is a margin of tolerance for the inconsistencies
of the environment". "To be in a good health means being able
to fall sick and recover". Tolerance is discussed in the chapter
on "Health measure".
In the present discourse health is a WOB signal unrelated to tolerance.
The
French physician Leriche said: 'Health
is life lived in the silence of the organs' (1). Only WOB indicates to the mind when it is sick. A silent WOB is healthy.
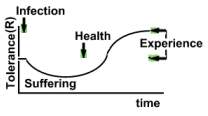
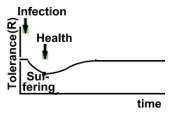
Tolerance is a measure for patient's
reserves. The image below depicts schematically a tolerance of an untreated
infection. Initially tolerance declines and when patient recuperates it raises.
Please note that health is unrelated to tolerance.
Health is regained when WOB regains control and stops complaining.
 |
 |
Mind disease
Training requires motivation to endure suffering, and motivation is a property of the mind. Some patients may suffer even their illness is negligible.
When treating a patient the physician ought to consider also the mind which
transmits to WOB how society regards its particular disease. Mind's attitude to infection
is called mind disease,
(here mind infection). A negative attitude raises anxiety which wastes resources and declines tolerance.
Mind disease in AIDS is far more risky than in sore throat.
Early treatment reduces anxiety, and renders mind disease milder.
WOB may gain more from an untreated infection, yet mind refuses to accept
WOB solution and insists on a better life. Physician has to
work out a compromise between WOB solution and mind demand.
Therapeutic margin of a drug
Two processes determine the evolution of
an infectious disease: Driver, and WOB (solution). Therapy has to consider both. Antibiotics
treat the driver. When antibiotics slow down microbe proliferation, WOB needs
less resources to withstand the invader. Then come measures to support WOB, like aspirin for reducing excess temperature. Driver
treatment may be somewhat toxic to WOB, which will require additional supportive
measures to avert driver toxicity. Like over-hydration to protect the kidney.
The benefit or harm (negative benefit) of a treatment depends on its effect on tolerance. The therapeutic margin of a drug, like an antibiotic is generally defined by the ratio potency / toxicity. Here the therapeutic margin is defined
by its effect on tolerance. If raising tolerance it is acceptable, and vice
versa. A therapeutic margin of a drug may be raised by supporting WOB against
drug toxicity. Like the above mentioned over-hydration which by protecting
the kidney, reduces tolerance decline, and widens the
therapeutic margin of the antibiotic.
Antibiotic treatment is an experience
Let's return to the untreated patient mentioned above. By
withholding antibiotics from the patient, WOB is protected from their toxicity.
On the other hand, antibiotic treatment is a WOB experience which may assist
it to handle future infections requiring
antibiotics. Such a reasoning
highlights the importance of tolerance and WOB experience when planning therapy.
Chronic uneventful disease
In most chronic diseases the driving process is unknown. However
its intensity can be inferred from WOB behavior. The disease evolves from one WOB solution to another, always
maintaining homeorhesis (homeostasis). At any instant WOB controls the disease,
only its resources (tolerance) decline. Since the driver is unknown and cannot
be eliminated like in infections, therapy is directed to slowing
down disease progression, which means
to slow down resource depletion
and maintain an adequate body
function
From the medical perspective, declining resources drive
the chronic disease ( D(i) ) and the formula describing disease progression
remains the same. R(i+1) = {D(i), W(I), M(i)}. Each of the three components
has to be considered.
1. Resource depletion D(i)
The amount of resources in the body depends on their input (uptake) and output (utilization).
Input
Therapy starts with a balanced diet.
Some resources may be particularly vital. Other may be depleted at different
rates. Medicine favors specific replacement of missing substances like vitamins
and hormones which has two drawbacks: 1. Hormone replacement
impedes internal hormone production. 2. The optimal dose
is generally unknown and may vary as disease progresses, so that even
a small dose may be toxic. Like during a sub clinical kidney weakness which
is not yet an overt failure.
A balanced diet lets WOB choose
whatever it needs. Any other routes of
resource replacement like injections, or infusions, ought to be postponed
as much as possible. This approach is meant far an uneventful disease progression. In acute conditions
an aggressive and invasive approach might be necessary.
Output
In most chronic diseases many missing substances are unknown, and when they
cannot be replenished with food, treatment ought to improve their utilization.
Like in angina pectoris. (see also WOB
boosting , when the patient suffers from a relative (internal)
oxygen deficiency. Gradual and careful sport
activity strengthens his
respiratory muscles, and improves oxygen input. Activity trains the
body (WOB) to utilize oxygen more efficiently. Its output (utilization) declines and
so does oxygen deficiency.
Resource diversion
When the above measures are exhausted,
one may attempt to divert resources from less vital organs to the more
vital. Fainting is such a measure. WOB eliminates the mind (consciousness),
patient faints, periphery requires less oxygen, and it is diverted to the
brain. This is also the rationale of putting a patient to bed. Or applying ancient Chinese martial arts to forward
dopamine to vital brain areas.
2. WOB boosting
W(i)
As disease progresses WOB learns to handle it better, and becomes more efficient,
which is most pronounced in cancer. Hazard rate is the
epidemiological manifestation of tolerance. When tolerance declines, hazard
rate rises and vice versa. It
is striking that as cancer progresses its hazard
rate declines. The longer the patient lives the better
his chances to survive. Since however his tolerance declines he ultimately dies. In other words,
the outcome of cancer depends on two factors, WOB boosting, and tolerance.
Although WOB learns to slow down tolerance decline, by itself it is
unable to replenish resources, and patient
dies.
A Cancer-Yogi trains her WOB to save resources, and slows down cancer progression, which may be expressed
metaphorically that she puts her cancer to sleep .
3. Mind M(i)
Mind depends on how the society faces a particular disease (R(i)). The prevailing
notion that cancer is a death sentence makes the patient with a minute tumor miserable, in spite of the fact that WOB is silent and she is healthy. Her
misery is called mind
cancer. At this stage of her disease
it poses a greater threat than WOB cancer. Now meditation
or guided imagery are extremely efficient.
Placebo is an effective measure
for many kinds of mind disease.
Etiology
The relationship between microbe and host illustrates how medicine views disease.
A disease is caused by an agent, which is regarded as etiology of this infectious disease. In
order to cure infection it suffices
to treat its etiology. Unfortunately in most chronic diseases etiology is unknown and medicine assigns
to such diseases an arbitrary etiology. For instance, replication
error is the etiology of cancer, or an error in the control of carbohydrate
metabolism is the etiology of diabetes.
Despite such a narrow and linear interpretation of disease,
the hunt after etiologies advanced medicine to its present state. Like the discovery of vitamins, hormones and antibiotics.
Ultimately medical science hopes to discover
etiologies of other diseases like cancer. Treatment will be better
yet the guidelines presented here will not change.
While medicine regards the organism as a complex linear machine, in reality it is extremely complex and non linear. It cannot be reduced to its elements and
has to be treated as a whole composed of a Driver, WOB and Mind.
Reference
1. Canguilhem G. Le normal et le pathologique.
translated into English by Fawcett CR, Cohen RS. Zone Books New York 1991
p 91.
|
The complete model: R : Resources During embryogenesis M is the placenta |