 |
G.Zajicek
In: New Frontiers in
Cancer Causation.
OH Iversen, Editor p. 81-107
Taylor & Francis, Washington DC, 1993.
Introduction
This article has been revised. Some sections appear
under different headings and the reader is advised to start with the following
chapters::
1 Failure of the current dogma
Many
share an uneasy feeling that something is fundamentally wrong in our interpretation
of cancer. Our ignorance is generally attributed to insufficient information
that is necessary to comprehend cancer correctly and since patients
have to be treated anyhow, treatment is obviously inadequate. Such an attitude
however is not unique to cancer. It constitutes the central motto of medicine:
"To treat despite uncertainty", and yet it seems as if
in cancer these doubts are more pronounced than in any other chronic disease.
Obviously
we still do not understand cancer. On the other hand, do we understand
arteriosclerosis better? It kills more patients than cancer and
yet even if treatment has failed we are satisfied that the patient was treated
properly. Such a sense of self-confidence is not shared by the oncologist.
In spite of being armed with the most sophisticated means known in medicine,
he helplessly follows the patient into his grave. Take for instance the
guiding principle of cancer treatment, according to which cancer is a parasite
originating in a chance event, transforming a healthy cell into a fierce
crab, proliferating without restraint until destroying its host . This parasite
should obviously be eliminated as soon as possible. And yet despite
its simplicity, this guiding principle fails to cure most patients.
Twenty
years after "launching the war" on cancer, leading specialists
admitted that the war is being lost (1-3). The National Cancer Institute
(NCI) has spent more than $1 billion on breast cancer alone and yet breast
cancer mortality does not change. Despite intensive effort to eradicate
the parasite upon its detection, from 1930 till 1988, age adjusted
mortality of breast cancer has remained virtually constant (4,5).
Fifty eight years of continuous debates about the preferred treatment of
breast cancer failed to improve the patient's life prospect. Failure is
attributed to micro-metastases that have spread prior to tumor detection,
yet patients with breast cancer may carry micro-metastases for years
without any clinical manifestations (6).
 |
Treatment
failed since it is based on false premises. It reflects a failure
of medical reasoning that seems adequate for all diseases except cancer.
It is presumed here that the necessary information for understanding
cancer exists and is wrongly interpreted.
The present
discourse introduces a new cancer paradigm according to which cancer
is a metabolic deficiency that ends in cachexia. The main task of
neoplasia is to aleviate the deficiency and prevent cachexia.
2 Cancer starts as a systemic illness
There
is more to cancer than just the crab. Two hallmarks of cancer, cachexia, and para-neoplasia, are usually ignored
since it is assumed that they are caused by neoplasia (8). In some cases
it appears as if cachexia and para-neoplasia accompany the tumor, yet usually
weight loss does not correlate with the type of cancer and its
duration, nor with the site or number of metastases (9). Weight loss is
one of the earliest manifestations of malignancy (10), and cachexia can
appear in patients with tumors that are less than 0.01% of the total body
weight. (11) Also para-neoplasia is unrelated to tumor size, location, or
the degree of metastasis, and may antedate the discovery of the tumor
by weeks , months, or even years (12). In spite of this, oncology
maintains that neoplasia is the primary factor in cancer, and systemic
effects are secondary. But, what if it is the other way around, and
cancer is first of all a cachexia accompanied by neoplasia?
At least this could explain why in most cancers treatment
fails.
Above
all, modern oncology maintains that host is defenseless against
its tumor and has to be screened and monitored otherwise he is doomed to
die. This conceptual impasse is highlighted by a title of a
recent book on cancer: "Contrary to Nature" (13). For centuries
physicians were trained to regard nature as their ally. The maxim
"while Medicine heals, only Nature cures" was unfortunately abandoned
by modern medicine. One has only to consider the profound complexity of
the human organism in order to realize that the most one may hope
to achieve, is to assist the organism in helping itself. Such
a modesty toward the organism that guided our forefathers was abandoned
by modern medicine, which should be regarded as root of the
oncological failure. If cancer appears as contrary to nature it is wrongly
comprehended and has to be reinterpreted so as to remain in accord with
nature.
3 The example of pernicious anemia
Cancer
is a disease of vertebrates induced by carcinogens that initiate a
metabolic deficiency manifested by para-neoplasia and cachexia.
Neoplasia is regarded here as a protective strategy mobilized by the
organism to repair a metabolic deficiency. During the pre-clinical
phase of cancer, deficiency is slight and compensated even by
a minute tumor. With time it gets worse and the tumor has to grow
more and more in order to make up for the loss, causing pain and secondary
damage to vital functions. The patient seeks help and
the disease starts its clinical course (14). When the deficiency becomes
pronounced, patient dies in a state of decompensation, known as
crisis or relapse.
There
is a disease called pernicious anemia that illustrates how neoplasia
might be protective. It is triggered by a "carcinogen" preventing
the entry of vitamin B12 into the body. During its pre-clinical phase,
that lasts about two years, the patient is healthy. The clinical phase
starts with anemia and "para-neoplasia", known
as combined degeneration of the spinal cord and brain. The bone marrow
displays "neoplastic" features, e.g., hyperplasia, maturation
arrest, and ineffective erythropiesis, that were regarded in
the past as "pseudo-leukemia" (15). These are protective
strategies of the bone marrow that keep the patient alive. With time the
deficiency deepens more and more until reaching the state of decompensation
whereupon the patient dies .
Cancer
is viewed here as pernicious
cachexia induced by the loss of a vital metabolite that is secreted
by stem cells and compensated by neoplasia.
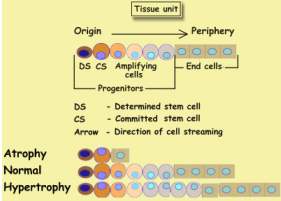
4 Streaming organism
The organism
is composed of myriads of cell streams that maintain homeo-rhesis.
Each stream represents one tissue unit that is nourished by
a determined stem cell (DS). All cells except stem
cell are transitional and their life span limited. Only the stem cell pool
exists as long as the organism does.
 |
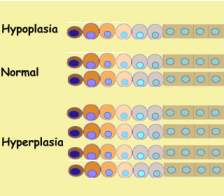 |
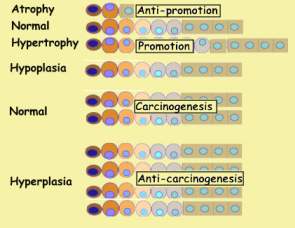
5 Unit hypertrophy and hyperplasia
Tissue units may enlarge by accumulating transitional cells, and when losing them they shrink. The two conditions are called respectively hypertrophy and atrophy (or hypotrophy). Unit hyperplasia occurs when entire units multiply, e.g., during growth. Bowel mucosa of the growing child elongates by forming new crypt units. First the determined stem cell in the mother crypt divides symmetrically, and generates an additional determined stem cell that forms a crypt bud. The bud elongates and finally forms a new crypt. Each new unit adds one cell to the pool of determined stem cells. During hypoplasia, stem cells die and units disappear.
6 The adult organism is incapable of increasing its stem cell pool.
In the adult hardly any new units are formed, and when destroyed they are replenished extremely slowly. Following small bowel resection, the remaining crypt-villus units become hypertrophic while hardly any new units are formed. Unit hypertrophy is the main compensatory mechanism of the adult in case of unit loss. On the other hand, the growing child is capable of replenishing lost units by new ones.
7 Cancer starts by stem cell depletion
The proposed
metabolic deficiency of cancer starts with stem cell depletion. Any
agent that destroys stem cells is a carcinogen. Stem cell depletion triggers
neoplasia in the same way as necrosis invokes inflammation. Stem cells secrete a substance 'A' that
is essential for the maintenance of transitional cells. When in the adult,
stem cells are lost there ensues a deficiency of substance 'A'. Since
stem cell replenishment is sluggish, the organism activates a salvation strategy in form of the
neoplasm for replenishing the loss. The neoplasm secretes a substitute,
called 'B', and restores the reversible deficiency.
During the pre-clinical phase of cancer the deficiency
is slight and compensated even by a minute tumor. With time it gets
worse and in order to make up for the loss the tumor has to grow more and
more, causing pain and secondary damage to vital functions. The patient
seeks help and the illness starts its clinical course. When
t deficiency becomes pronounced, the patient dies in a state
of de-compensation, known as crisis or relapse.
Neoplasia is a life saving process yet
in an advanced stage it may cause damage , exactly as inflammation, also
a life saving process that may also cause secondary damage. While inflammation
repairs tissue damage, neoplasia repairs stem cell deficiency.
When cancer advances, secondary damage by tumor predominates, which gave
cancer with its crab metaphor
8 Deficiency promotion
Two
factors determine the intensity of the 'A' deficiency, Stem
cell depletion by carcinogens, and its uptake rate by transitional
cells. Agents that increase 'A' uptake by transitional cells
are called promoters. Hormonal imbalance is a powerful deficiency
promoter. It was demonstrated in a classical experiment in which ovarian
tissue was transplanted into the spleen of castrated mice (23). Usually
the secretion of pituitary gonadotrophins is modulated by steroid hormones
that are secreted by the ovary. When transplanting the ovary into the spleen,
steroids are metabolized by the liver and do not reach the pituitary. In
the absence of hormonal feedback more and more gonadotrophins are secreted
stimulating the transplanted tissue to proliferate until turning malignant.
Since hormones do not deplete stem cells they are not carcinogenic. On the
other hand, hormone overproduction increases the pool of transitional
cells that utilize more of the stem cell product, promoting
a deficiency, that is later compensated by ovarian neoplasia.
9 Anti-promotion
Processes
operating in cancer are balanced and reversible. For each process there
exists an anti-process operating in the opposite direction. Any agent
the diminishes the consumption of the stem cell metabolite by transitional
cells is an anti-promoter. Anti-promotion is applied in the treatment
of patients with disseminated breast cancer. Previously they were castrated
and their adrenals removed. Today the same is achieved with
hormonal analogues and irradiation. These procedures reduce
the pool of transitional cells in the breast glands. The cells consume
less of 'A' and its 'B' substitute, the deficiency declines, the demand
on the neoplasm diminishes, and it shrinks. By reducing the transitional
cell pool, these measures act as anti-promoters.
 |
10 The main benefit of chemotherapy is its anti-promotion.
Chemotherapy
is carcinogenic, since depleting normal and neoplastic stem
cells. It is also an anti-promoter, since eliminating proliferating
transitional cells. The outcome of chemotherapy
treatment depends on its effect on each feature. Proliferating target
cells are the most sensitive to chemotherapy, then come tissue stem cells
and the least sensitive are neoplastic stem cells. When the patient is first
treated, chemotherpy reduces its proliferating transitional
cells (anti-promotion) and the deficiency is ameliorated. Yet
since chemotherapy depletes also stem cells and reduces the tumor, the relief
is brief, the deficiency deepens and the neoplasm enlarges.
Since tumor stem cells are most resistant to chemotherapy, this therapy
is more harmful to 'A' secreting stem cells than to the tumor, and the illness
becomes resistant to chemotherapy.
Anti-promotion
seems to be also the main benefit of adjuvant chemotherapy in
breast cancer. The drug poisons first the ovary and pituitary,
reducing their hormonal output, the breast tissue shrinks, the
deficiency declines and the neoplasm shrinks. The relative sizes of the
two cell pools, stem and transitional, determine the state of the metabolic
deficiency in cancer.
11 Anti-carcinogenesis
Any agent
that increases the stem cell pool is anti-carcinogenic, e.g., unit hyperplasia
during organ growth. The child, unlike the adult, can restore
its deficiency by forming new 'A' producing stem cells. Childhood cancers
are therefore more benign than adult cancers and respond better to therapy. Most
childhood cancers are actually congenital malformations induced by teratogens.
Generally teratogens cause malformations yet when depleting also stem
cells malformations are accompanied also by cancer.
12 Congenital neoplasia
Congenital
tumors generally present themselves as poorly differentiated cell masses,
growing more rapidly than most adult tissues do, and yet many regress
spontaneously (24). Of the 29 cases
of spontaneously regressing neuroblastomas documented by Everson
and Cole (25), 21 were detected in infants under 6 months of age. The younger
a child with a neoplasm the better its chances to be cured since its
anti-carcinogenic potential is the greatest. The estimated cure rate of
neuroblastomas among neonates is about 62-70%, while after the age of two,
only 5% are curable (26). This "oncogenic period of grace beginning in utero and extending through the first
months of life" (27), reflects the anti-carcinogenicity of normal
growth.
13 Trophic effect of neurons
The incompetence
of the adult to replenish his missing stem cells is puzzling. Particularly
since the same stem cells when grown in vitro proliferate vigorously
and may even become immortal. Stem cell proliferation is restrained
by the nervous system.
The nervous
system is best known as action potential carrier. Yet neurons
participate also in the metabolism of their target organs. This
function is known as trophic effect of the neuron (28) and
was first demonstrated in the regenerating newt limb (29). Following
limb amputation the stump is invaded by undifferentiated pluri-potential
stem cells called blastema that gradually differentiate into a new limb.
This process depends upon nerve supply. It fails if local
nerves were removed. On the other hand if the local nerve supply was left
intact and and the contra-lateral nerve trunk sutured into the blastema
region, the limb regenerates faster.
Similar
trophic effects modulate the metabolism of muscles, or control the differentiation
of taste buds (28). Apparently the nervous system modulates the
metabolism of all organs in the body as well as their stem cells and
restrains them from forming new tissue units. This trophic effect
is poisoned by carcinogens that initiate the postulated 'A' deficiency
and cancer.
14 Cancer as neural disease
It is
proposed that stem cells are depleted also by a carcinogen induced
neuropathy. This possibility was raised under different circumstances
by Janet McCredie who studied thalidomide induced phocomelia (30, 31). McCredie postulated that differentiation in the embryo is
under neurotrophic control. Thalidomide induces a neuropathy
and neuron death that is manifested later by malformations. The same
trophic relationship operates also in cancer. Para-neoplasia is an
extended neuropathy that ends in cachexia and is compensated by neoplasia.
15 Cancer treatment
Carcinogen
prevention is the best cancer treatment. When deficiency ensues it should
be treated by replacement of the missing 'A' substance or its 'B' substitute.
Since each tissue grows a different neoplasm each cancer ought
to be treated by the appropriate stem cells. Potential stem cell
sources are animals or humans whose stem cells can be enriched
in vitro.
Until
the missing substance has been isolated, treatment should be directed to
maintain neoplasia and correct its secondary manifestations. When
secondary sequelae dominate the clinical picture, they have to be treated
even if it damages the stem cell pool As deficiency progresses, one
has to turn to anti-promotion measures, e.g., endocrine ablation, or chemotherapy.
Chemotherapy has to be applied sparingly, and its dose
titrated in the same way as done during digitalization, raise it
until mild poisoning has been achieved, and not more.
It may
seem strange that even cachexia contributes to the patient's well being. In spite his poor condition the patient maintains
a delicate balance with his illness and his state proceeds an optimal course
under the given circumstances. Cachexia is manifested by the depletion
of transitional cells and acts therefore as anti-promoter.
16 Carcinogenesis by organ resection.
Organ ablation is a carcinogen. Several studies have demonstrated
that organ resection is followed by an increased tendency to contract
cancer in the treated organ. In one study, 6.5% percent of patients
that had gastric surgery for benign conditions returned after five years
with gastric stump carcinoma (41). A significantly increased mortality
was detected also in a cohort of patients that had partial gastrectomy
for benign conditions (42). Partial colon resection promotes cancer growth
in rats (43). Sprague-Dawley rats were treated with dimethylhydrazine for
three months. After a treatment free period of five months, their colons
were resected with an end-to-end anastomosis. One year after discontinuation
of the carcinogen, and seven months after surgery, 50% had anastomotic
tumors .
Partial
hepatectomy accelerates hepato-carcinogenesis (44)
by reducing the stem cell pool, since the regenerating liver does
not produce new units and compensates for the loss by unit hypertrophy.
17 Inflammatory cancers
While
in some esoteric cancers, e.g., Hodgkin's disease, seminoma, osteosarcoma,
childhood leukemia, yield to massive irradiation or chemotherapy,
the overwhelming majority of cancers does not respond to this kind of treatment
since adult cancers become resistant to chemotherapy. Resistance to chemotherapy
is a hallmark of cancer and main reason for treatment failure. This
feature may be regarded as a pathognomonic of cancer so that
if a tumor yields to chemotherapy it is non cancerous.
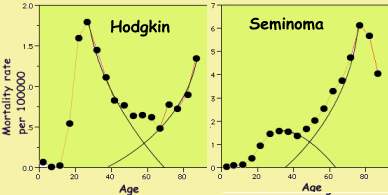 |
18 Hodgkin's disease
Hodgkin's
disease, is the only cancer that called a disease, indicating that it behaves
in a different way than genuine cancers. Some authors suspect that
it starts as granulomatous inflammation ending as lymphoma, being
predominantly granulomatous in young adults while in patients over
50 years, it is a lymphoma (45). Its age specific mortality curve exhibits
a distinct a shoulder that accounts for a population of young
adults with the so called "benign" Hodgkin's disease
generally localized and). From the age of 50 year the curve ascends nearly
exponentially and could represent patients with genuine lymphoma
with features of malignant lymphosarcoma. In 284 patients with Hodgkin's
disease, Reed-Sternberg cells, eosinophils and the extent of fibrosis were
more pronounced in young adults, while atypical mitoses and other features
of malignancy were more common in older persons (46). The authors were struck
also by the epidemiological similarity between Hodgkin's disease and multiple
sclerosis, suggesting that both could result from a very prevalent infection
of low pathogenicity which is characteristic also of poliomyelitis (47).
19 Seminoma
In seminoma
the first peak is even more pronounced. Most seminomas exhibit a clear
inflammatory component, e.g., lymphocytic infiltration and granulomatous
reaction (48). It appears as if seminoma, Hodgkin's disease, osteosarcoma
and connective tissue sarcomas, start as inflammatory diseases and
only later turn into malignancies. Apparently total lymphoid irradiation
and chemotherapy are effective only in their infective phase
and less in their neoplastic stage exactly as in non-Hodgkin lymphomas.
These neoplasms are better called inflammatory cancers.
The dramatic
response to therapy of childhood cancers and leukemia is ascribed here to
the anti-carcinogenic potential of the growing organism.
Cancer
is a metabolic deficiency! (50) This
is the modern interpretation of Hippocrates’ 38th aphorism:
"It is better not apply any treatment in cases of occult cancer; for
if treated, patients die quickly; but if not treated, they hold out
for long time" (51).
20
Summary
According to the current dogma cancer is a
parasite originating in a chance event, transforming a healthy cell into a
fierce crab, proliferating without restraint until destroying its host. In
spite of its simplicity, this guiding principle fails to cure most patients.
Treatment fails since it is based on false premises. It is presumed
here that the necessary information for understanding cancer is known and
is wrongly interpreted.
Cancer is a metabolic deficiency, that
starts with stem cell depletion. Stem cells secrete a substance 'A'
that is essential for the maintenance of transitional cells. Since in
the adult stem cell replenishment is sluggish, the organism activates
a salvation process in form of the neoplasm for replenishing the loss.
and restores the reversible deficiency. With time deficiency
gets worse. In order to make up for the loss the tumor has to grow more and
more, causing pain and secondary damage to vital functions. Cancer is viewed
here as pernicious cachexia induced by the loss of a vital metabolite
produced by stem cells and compensated by neoplasia.
Two factors determine the intensity
of the 'A' deficiency, stem cell depletion and its uptake rate by
transitional cells. Carcinogens initiate stem cell depletion,
while anti-carcinogens restore it. Promoters increase 'A' uptake by
transitional cells and anti-promoters decrease it. Stem cells are depleted
also by a carcinogen induced neuropathy.
Diseases, e.g., Hodgkin's disease, seminoma,
connective tissue sarcoma start as inflammations that become
malignant. Chemotherapy is effective only during their inflammatory
phase. The favorable response of childhood cancer to therapy results from
the capability of the growing organism to replenish lost stem cells.
21 Synopsis
1 The failure of the current dogma
According to the current dogma cancer is a parasite originating in a chance
event, transforming a healthy cell into a fierce crab, proliferating without
restraint until destroying its host . This parasite should obviously be eliminated
as soon as possible. And yet in spite of its simplicity, this guiding principle
fails to cure most patients.
2 Cancer starts as a systemic illness
Oncology maintains that neoplasia is the primary factor in cancer, and
that para-neoplasia and cachexia are secondary. Here it is proposed that cancer
is first of all a cachexia initiated by para-neoplasia and compensated
by neoplasia.
3 The example of pernicious anemia
Cancer is viewed here as pernicious cachexia induced by the loss of a vital
metabolite that is secreted by stem cells and compensated by neoplasia.
4 Streaming organism
The organism is composed of myriads of cell streams that maintain homeo-rhesis.
Each stream represents one tissue unit that is nourished by a
determined stem cell.
5 Unit hypertrophy and hyperplasia
Tissue units may enlarge by accumulating transitional cells, and when losing
them they shrink. The two conditions are called respectively hypertrophy
and atrophy (or hypotrophy). Unit hyperplasia occurs when entire units
multiply , e.g., during growth.
6 The adult organism is incapable of increasing its stem cell pool.
While a growing child is capable of creating new tissue units, and replenishing
lost units with new ones. In the adult this facility is either lost,
or extremely reduced .
7 Cancer starts with stem cell depletion
The postulated metabolic deficiency of cancer starts with stem cell
depletion. Any agent that destroys stem cells is a carcinogen. Stem cells secrete a substance 'A' that is essential
for the maintenance of transitional cells. When in the adult, stem cells are
lost the organism activates a salvation strategy in form of
a neoplasm that secretes a substitute called 'B'.
8 Deficiency promotion
Agents that increase 'A' uptake by transitional cells are called
promoters.
9 Anti-promotion
Any agent the diminishes uptake of the stem cell metabolite by transitional
cells is an anti-promoter.
10 The main beneficial effect of chemotherapy is due to anti-promotion.
When the patient is first treated, chemotherpy reduces its proliferating
transitional cells (anti-promotion) and the deficiency is ameliorated.
Yet since chemotherapy depletes also stem cells (carcinogenesis), the
relief is brief. Deficiency deepens and the neoplasm enlarges. Anti-promotion
is also the main benefit of adjuvant chemotherapy in breast cancer.
11 Anti-carcinogenesis
Any agent that increases the stem cell pool is anti-carcinogenic, e.g., unit
hyperplasia during organ growth. Most childhood cancers are actually
congenital malformations induced by teratogens. Generally teratogens
cause malformations yet when depleting also stem cells, malformations are
accompanied by cancer.
12 Congenital neoplasia
The younger a child that carries a neoplasm the better its chances to
be cured since its capacity to form new units (or anti-carcinogenic
potential) is the greatest.
13 Trophic effect of neurons
The nervous system modulates the metabolism of all organs in the body as well
as their stem cells. . This trophic effect is poisoned by carcinogens
that initiate the 'A' deficiency and cancer.
14 Cancer as a neural disease
Carcinogen induced neuropathy initiates cancer by stem cell depletion and
is clinically manifested as para-neoplasia.
15 Cancer treatment
Carcinogen prevention is the best cancer treatment. Then comes replacement
of the missing 'A' or its 'B' substances. Finally, anti-promotion. Even cachexia
has some beneficial aspects, since acting as anti-promoter.
16 Carcinogenesis by organ resection.
Gastric surgery for benign conditions is accompanied by an increased tendency
to get gastric stump carcinoma. Partial colon resection promotes cancer growth
in rats. Partial hepatectomy accelerates hepato-carcinogenesis. Since
removing stem cells these procedures are carcinogens.
17 Inflammatory cancers
At least some esoteric cancers, e.g., Hodgkin's disease, seminoma, osteosarcoma,
childhood leukemia, yield to massive irradiation or chemotherapy. Yet
resistance to chemotherapy is pathognomonic of cancer, so that
if a tumor yields to chemotherapy it is non cancerous.
18 Hodgkin's disease
Starts as chronic inflammation (granuloma) and ends as lymphoma. Chemotherapy
is effective only in the first stage.
19 Seminoma
Most seminomas exhibit a clear inflammatory component, e.g., lymphocytic
infiltration and granulomatous reaction. It appears as if seminoma, Hodgkin's
disease, osteosarcoma and connective tissue sarcomas, start as inflammatory
diseases and only later turn into malignancies. The dramatic response to therapy
of childhood cancers and leukemia is ascribed here to the anti-carcinogenic
potential of the growing organism.
22
References
1. Marshal E. Breast Cancer:
Stalemate in the war on cancer.
Science
254:1719-1720,1991.
2. Zajicek G. Progress against
cancer: are we winning the war?
Cancer
J. 3:2 ,1990
3 Zajicek G. Cancer
wars
Cancer
J. 4:4,1991
4 McKay FW, Hanson MR,
Miller RW. Cancer mortality in the U.S: 1950-1977
NIH Publication
No. 82-2435, 1982
5 Silverberg E, Lubera
J. Cancer statistics.
CA -A Cancer Journal for Clinicians 40:16-17,1990
6 Zajicek G. Long survival
with micrometastasis. At least 9% of breast cancer
patients carry metastases more than 10 years.
Cancer
J. 1:414-415,1987
8 Zajicek G. Hypothesis:
cancer is a metabolic deficiency
Cancer
J. 4:356,1991
9 Theologides A. Cancer
cachexia.
Cancer
43:2004-2012,1979
10 Theologides A. Pathogenesis of
cachexia in cancer.
Cancer
29:484-488,1972
11 Tisdale MJ. Cancer cachexia.
Br J. Cancer
63: 337-342,1991
12 Payan HM, Gilbert EF, Mattson
M. Hematological and biochemical paraneoplastic disorders. Arch. Path.Lab
Med. 102: 19-21,1978
13 Shimkin MB. Contrary to nature.
DHEW Publ.
No. NIH 76-720, 1977.
14 Zajicek G. What is neoplasia?
Cancer
J. 4:228,1991
15 Wiernik PH Acute promyelocytic
leukemia: another pseudoleukemia?
Blood 76:1675-1677,1990
23 Pitot HC. Endogenous carcinogenesis:
The role of tumor promotion.
Proc Soc.
Exp. Biol. Med. 198:661-666,1991
24 Zajicek G. Congenital Neioplasia:
A stem cell pathology.
Medical
Hypothes. 16:303-313,1985
25 Everson TC, Cole WH. The spontaneous
regression of cancer
WB Saunders
Philadelphia PA. 1966
26 Bolande RP. Developmental pathology
Am. J.
Pathol. 94:627,1979
27 Bolande RP. Teratogenesis and
oncogenesis,
In Handbook
if Teratology. Eds Wilson JG, Fraser PC.
Vol 2 p
293-325,1977
28 Guth L. Trophic effects of vertebrate
neurons.
Neurosci.
Res. Bul. 7: 1-30, 1969
29 Singer M. Neurotrophic control
of limb regeneration in the newt/
Ann. N.Y.
Acad. Sci. 228: 308-312,1974.
30 McCredie J Embryonic neuropathy.
A hypothesis of neural crest injury as the
pathogenesis of congenital malformations. Med J. Aust. 1:159-163,1974
31 McCredie J, North K, de Iongh
R. Thalidomide deformities and their nerve
supply. J. Anat. 139,397-410,1984
41 Giarelli L, Melato M, Stanta
G, Bucconi S, Manconi R. Gastric resection:
A high
frequency of gastric carcinoma. Cancer 52:1113-1116,1983
42 Offerhaus GJA, Tersmette AC,Huibregste
K, van de Stadt J, Tersmette KWF, Stijnen TH, Hoedemaeker PJ,
Vandenbrouke JP, Tytgat GNJ. Mortality caused by stomach cancer
after remote partial gastrectomy for benign
conditions.
Gut
29:1588-1590,1988
43 Rubio CA, Nylander G, Wallin
B, Sveander M, Alun ML, Duvander A.
Partial
colon resection as promotor of cancer growth in the rat.
J. Surg.
Oncol. 27:236-238,1984
44 Rotstein J, Macdonald PDM, Rabes
HM, Farber E. Cell cycle kinetics of rat
hepatocytes in early preneoplastic lesions in hepatocarcinogenesis.
Cancer
Res. 44:2913-2917,1984
45 MacMahon B. Epidemiology of Hodgkin's
Disease.
Cancer
Res. 26:1189-1195,1966
46 Newell GR, Mills PK,Johnson DE.
Age differences in the histology of Hodgkin's
disease. Natl Canc. Inst. J. 45:311-316,1970
47 Newell GR. Etiology of multiple
sclerosis and Hodgkin's disease.
Am. J.
Epidemiol. 91:119-124,1970
48 Mostofi PK, Price Jr EB. Tumors
of the male genital system.
Armed Forces
Inst. Pathol. 8:28-100,1970
50 Zajicek G Cancer is a metabolic
deficiency
Medical
Hypoth. 21:105-115, 1986
|
Physician
|
Philosopher
|
||
|
Click on your icon
to follow your trail
|
|||