Tissues are composed of tissue units. The tissue unit consists of a stem cell
(DS) whose progeny are dividing progenitors, which mature
to non dividing end cells. Progenitors and end cells are collectively
called transitional cells. A tumor is initiated in a single
tissue unit when a normal stem cell is transformed
into a neoplastic. Obviously this transformed cell has to be a stem cell (DS),
since transformed transitional cells are short lived. Tumor
initiation is a stem cell event.
During the initial stages of tumor development the tissue unit elongates and
is populated mainly by progenitors. The ratio end cells
/ progenitors declines until all end cells disappear
and the entire unit proliferates.
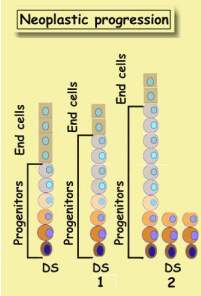
During the subsequent phase neoplastic stem cells populate the entire unit.
The gradual loss of end cells is known as maturation
arrest.
Each stem cell creates its own neoplastic unit. Together they form a growing
tumor. These are the earliest changes in neoplastic (or tumor) evolution.
They are called also precursor
lesions,
exhibiting the salient features of a tumor. Progenitor
amplification and neoplastic stem cell accumulation.
As neoplastic cells evolve they lose
their original stem cell attributes,
acquire new gene mutations which endow them with new neoplastic properties.
This process is called de-differentiation.
Mammary tumor evolution
The mammary gland unit proceeds through the same stages. Initially it is well
differentiated, populated with end cells containing estrogen receptors which
make it sensitive to estrogen. The hormone promotes its growth while castration
retards it. During this period the tumor is estrogen
dependent.
As it evolves it gradually loses
its end cells with their receptors,
and becomes estrogen receptor negative. Now it grows even in the absence of
estrogen. This process is known as de-differentiation.
Tamoxifen effect
Tamoxifen
selectively inhibits the effects of estrogen on breast tissue, provided it
has estrogen receptors, otherwise it is much less effective. Khoshnoud
et al (1) studied the long-term pattern of disease recurrence among in pre-
and post-menopausal patients with primary breast cancer according to estrogen
receptor status. The study was based on patients with an operable, invasive
breast cancer entered in one of three controlled clinical trials conducted
by the Stockholm Breast Cancer Group. They selected those 2,562 patients who
had been randomly allocated between adjuvant tamoxifen and no adjuvant systemic
therapy. These patients had a known estrogen receptor status. The following
figures are reproduced from
the published paper and will be interpreted in terms of breast tumor kinetics.
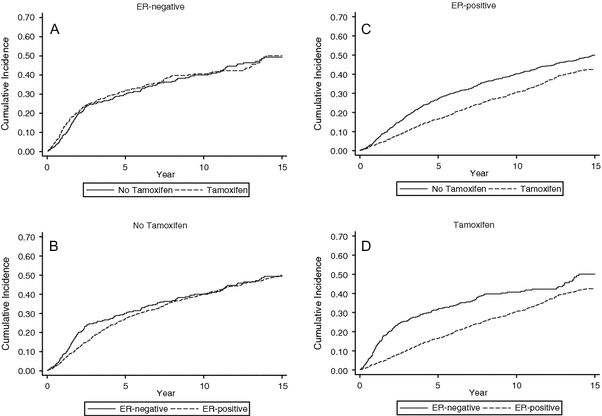
Fig.1 Cumulative incidence of events among all 2,562 patients according to
ER status and randomized treatment allocation (tamoxifen or no tamoxifen)
Interpretation
ER positive and negative tumors represent two stages in breast tumor evolution.
ER-negative tumors are less
differentiated and more advanced,
and do not respond to tamoxifen (Panel A). Thus the response to tamoxifen
(Panel C) indicates which patients carry a more differentiated tumor.
Initially the recurrence rate of ER-positive tumors is lower than that of
ER-negative (Panel B), and later on their recurrence rates coincide.
Cumulative incidence of ER-negative tumors (panel A) proceeds through
two periods. An accelerated when the incidence
curve is steep, and a decelerated when its slope becomes
more moderate. The slope is proportional to the rate of tumor recurrence.
The steeper the curve the faster tumors recur. More tumors recur during the
first three years than later on. This phenomenon is known as bi-modal hazard
(BMH). The
cumulative incidence is a manifestation of
the bi-modal hazard (BMH)
and is explained elsewhere.
BMH is most pronounced in ER-negative tumors (panel A) and less in ER-positive
tumors (panel B). Panel C illustrates that tamoxifen lowers the recurrence
rate only in ER-positive tumors and does not affect ER-negative tumors (panel
A).
Tumor growth rate
Tumor incidence is defined as recurrence of a previously hidden tumor which
depends on two factors: Resolution power of tumor detecting means, and tumor
growth rate. During the accelerated phase tumor grows faster and following
the third year its growth rate declines. Tamoxifen slows down ER- positive
tumor growth and does not affect the growth of ER-negative tumors
Tumor dormancy
The tumor incidence curve indicates that treatment did not remove all tumor
cells, and they continue growing. Initially faster and later on slower. Yet
what about a tumor that recurs after 10 years? Did it grow that slow? Or might
it rest there in a dormant state, known in cell kinetics as G-0 phase? What
kept it dormant so long? It is our belief that tumor dormancy was
sustained by the organism, which is discussed in other chapters
of this site
In summary: Tumor recurrence rate is proportional to tumor growth
rate.
Additional reading:
Streaming Tissues
Bi-Modal Hazard
Cumulative incidence
References
1. Mahmoud R. Khoshnoud , Tommy Fornander , Hemming Johansson and Lars-Erik
Rutqvist
Long-term pattern of disease recurrence among patients with early-stage breast
cancer according to estrogen receptor status and use of adjuvant tamoxifen
Breast Cancer Research and Treatment Volume 107, Number 1 / January, 2008